

Higher cognitive functions - so what does the brain actually do, and how do we know?
Higher cognitive functions - so what does the brain actually do, and how do we know?
Mahdiyyah Osman

I find the brain extraordinary! There is always something in some field of Neuroscience and Neuroanatomy which engages my curiosity.
But how does the brain actually work, what does it do, and how do we know? Let’s start simple.
The brain is divided into 2 halves - the right and left hemisphere. These are connected by what is called the corpus callosum - a thick strip of nerve fibres, allowing communication between the 2 halves.

The 2 halves of the brain are not exactly the same - this is termed cortical asymmetry. Cognitive processes are dominant on one side of the brain, and each hemisphere has a more specialised function. This asymmetry is not exclusive to us humans, and is actually common to both vertebrates and invertebrates. However, we as humans have the greatest cortical asymmetry compared with all mammals. It is because of this asymmetry that we have language, as well as many other higher cognitive specialisations and functions.
Professor Daniel Geschwind and Professor Christopher Walsh (at Harvard and UCLA Medical Schools respectively), have identified that some genes in our brain, which in turn code for proteins, are expressed asymmetrically. In the human fetal brain, they found that different genes are expressed on one side of the brain compared to the other, and also earlier on one side than the other. The significance of this is not yet fully understood but again highlights how either halves of our brain may be, in some way, suited to different things1.
So let’s discuss the different lobes of the brain. Each half of the brain is divided into 4 lobes. These are the frontal, parietal, occipital and temporal. Let’s take each one in turn.

The frontal lobe
The frontal lobe is vital to our consciousness and behaviour. It is the emotional control centre, as well as home to our own personality. It also includes motor function, spontaneity, language, problem solving, amongst other functions. Brain injury studies in the frontal lobe have alluded to its functions - for example, frontal lobe injury in patients has resulted in loss of fine movement and strength of arms, hands and fingers, as well as patients producing little spontaneous facial expressions, and being prone to language disorders such as Broca’s aphasia. This latter disorder occurs as the ‘Broca’s language centre’ is damaged, thus resulting in a partial loss of ability to produce language, whereas patients’ comprehension remains intact (also called expressive aphasia as they cannot express what they want to say properly).

A case
In the 1800s, a patient named Phineas Gage, a railroad worker, had an accident where an iron rod passed through his skull. It entered the left side of his face, and exited through the top of his head - thus completely lesioning his frontal lobes. He survived this, and lived for another 12 years. Through his case, scientists at the time were able to learn about the function of the frontal lobe. They learnt the effects on consciousness and behaviour - Gage could still learn, remember, sense and perceive his environment and execute motor functions well, but his personality changed completely. After his accident, based on questions asked to those around him, he was less polite, erratic, unreliable and offensive to others.

The Parietal lobe
The parietal lobe’s function is somatosensory. This means sensory perception and integration - not just the main senses such as hearing, sight, touch, smell and taste, but also pressure, pain, heat, cold, tension. Even the sense of touch can be categorised further into e.g. 2-point discrimination which means distinguishing between 2 points on your body without a visual stimulus. The parietal lobe is also vital for the sense of proprioception - your ability to determine where your body is in space, and be aware of this without constantly thinking about it. Examples of this include how we can walk without looking at our feet, or touch our nose even when our eyes are closed. The parietal lobe takes in the world and integrates this sensory information, so we understand what is going on.

Studies have shown that damage to the left parietal lobe leads to Gerstmann’s Syndrome. This is a rare disorder which entails loss of 4 neurological functions:
Inability to write - dysgraphia or agraphia
Loss of ability to do mathematics - acalculia
Inability to identity ones’s own or another’s fingers - finger agnosia
Inability to make the distinction between the right and left side of the body
as well as right-left confusion.
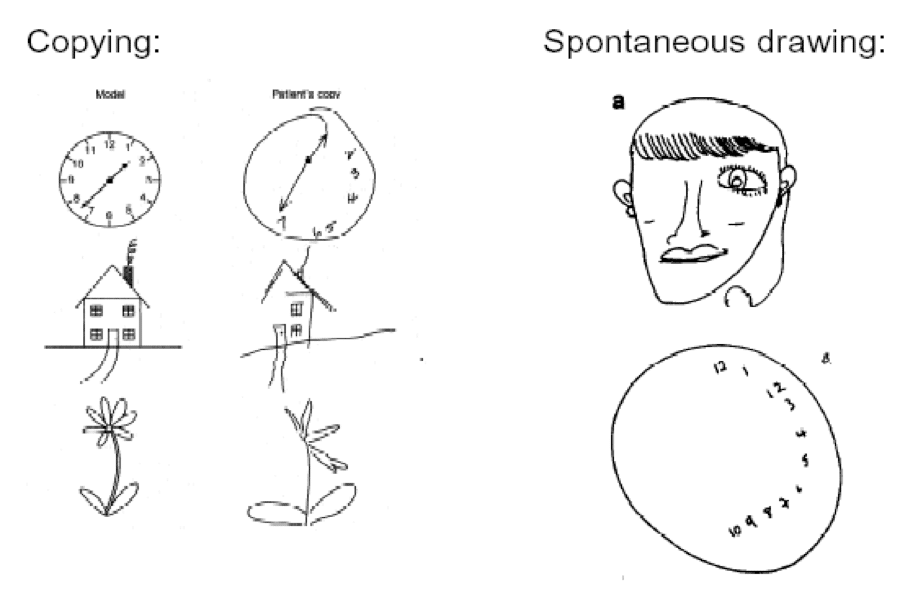
In contrast, damage to the right parietal lobe can cause neglect of part of the body and space - so this can impair dressing and washing, as well as difficulty making things, termed constructional apraxia. Constructional apraxia refers to the inability of patients to copy accurately drawings or three-dimensional constructions. Patients with right parietal lobe injuries also have denial of their deficits - anosagnosia, which is a lack of insight into, and ability to understand, their illness.
Right lobe injury symptoms manifest on the opposite side of the body to the corresponding brain lesion, so occur on the left side of the body. Right parietal lobe damage can also cause hemispatial neglect - this means neglecting the left side of the individual’s visual field. This is when individuals fail to be aware of items to one side of space, and it is characterised by reduced awareness of stimuli.


The temporal lobe
This lobe’s role is processing sensory input into derived meaning for memory, language and emotion. It contains the primary auditory cortex - the first area for interpreting information we gain from hearing sounds from our ears, giving it meaning. It allows selective hearing, so we are not focussed on all sounds surrounding us at any given moment, and can filter what is important and salient to us at the time. This is how we can ignore sounds on the tube when we’re focussed on reading or filter out noises in a crowded place and direct our attention to a friend speaking to us.

The temporal lobe also contains the limbic system - which is involved with our motivation, learning and memory, composed of the amygdala and hippocampus. The hippocampus is important for formation of short-term memories into long-term memories, and the amygdala is significant for emotional memory and expression.
Patients such as HM and Clive Wearing, who are well-known to Neuroscientists, have shown us its importance in memory formation. HM had temporal lobe epilepsy, and underwent surgery to remove parts of his right and left temporal lobe. The surgery was successful in reducing his seizures, however, HM lost the ability to form new long-term memories. This was the first evidence that the process of memory could be localised and attributed to certain regions of the brain. As a lot of his hippocampus was removed, it highlighted this area as central to conversion and formation of short-term to long-term memories.
In the case of Clive Wearing, he contracted a virus which attacked his brain - Herpes Simplex encephalitis. This meant he was unable to store new memories, as well as unable to control his emotions and associate memories well. His memory lasts between 7 and 30 seconds, so it basically resets his consciousness once the time span of his short-term memory is finished. So whenever his wife leaves the room and comes back in, he greets her as if he hasn’t seen her for years, or when he goes out dining, he can remember the name of the food, but cannot link it with taste as he has forgotten.
The limbic system is also important for autonomic functions such as sexual arousal, anxiety, hunger and thirst, amongst others. Damage to the amygdala can cause difficulty in learning the associations between certain stimuli and emotional states, so individuals cannot learn how a stimulus can predict reward or danger. Disruption to connections between the limbic system and other areas of the brain can present with individuals showing inappropriate emotional and social behaviour - despite no intellectual deficits, e.g. laughing at a funeral, or peeing in public.
In terms of language, our Wernicke’s area is located in our dominant side temporal lobe. This is an important region which is attributed to processing and giving meaning to verbal material (speech), as well as the written word. It helps us understand speech and language. As you can guess, damage to the left temporal lobe results in Wernicke’s aphasia, where patients can speak but not understand language.
The temporal lobe is important for complex visual recognition such as objects and faces, and damage to the right temporal lobe results in impaired memory for non-verbal material e.g. music and drawing, as well as prosopagnosia - an inability to recognise faces, or attribute someone’s identity to them. This does not in fact have to follow a brain injury or distinct damage to this area.
Oliver Sacks, a famous British Neurologist, describes in the Man Who Mistook His Wife for a Hat (the first Neuroscience book I ever read and my favourite!) a patient he comes across with prosopagnosia, after the patient sustained a brain injury. This is essentially ‘face blindness’. I was surprised to learn a few years later that Sacks' himself suffers with this. During his school days, he used to recognise his friends by utilising specific criteria - “Jonathan was tall and red-haired, Eric had thick spectacles, and thick eyebrows. Originally I recognised them by this, and then I came to recognise their faces, but I didn’t recognise too many other people”. This also extending to not even recognising himself through a mirror at one time. If you would like to find out more, I would highly recommend watching some of his Youtube videos - referenced below2.
Finally, the occipital lobe
At the back of the brain, this lobe is responsible for visual processing. It is connected to the retina in the eye via the optic nerve and optic tract, and contains the primary visual cortex (Brodmann area 17).

Damage to this area results in cortical blindness, otherwise known as visual agnosia - this is despite the eyes functioning normally. The information received from the outside world cannot be processed properly, and patients can experience visual field defects such as homonymous hemianopia
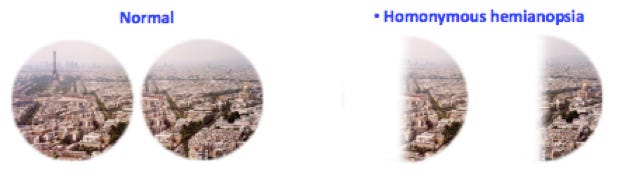
or different visual field defects, depending on which side and how much of the occipital lobe is injured.
Additionally, this area of the brain is significant for colour discrimination, so patients have a lack of this, being colour blind.
I hope you have gained a glimpse into how wonderful and incredible the brain actually is. Some things we don’t really think about - such as how we gain meaning from the world, the way our brain processes this, the ability to recognise a face, or draw joy from something we love, to name a few.
Let me know if you’ve enjoyed reading! And if you’d like to read more about a certain topic :)
- Mahdiyyah Osman, Anatomy Blog Director and 3rd Year Medical Student
https://dnalc.cshl.edu/view/1180-Cortical-Asymmetry-Left-Brain-Right-Brain.html
‘I Do Recognize My Friends: Oliver Sacks on Face Blindness’ and ‘Oliver Sacks: Face Blindness’ on Youtube